
5th Metatarsal Avulsion Fracture (Pseudo-Jones Fracture)
Summary
5th Metatarsal Avulsion Fracture Handout
A twisting injury to the ankle and foot may cause an avulsion (pulling off) fracture of the base of the 5th metatarsal – the bone that attaches the little toe to the midfoot (Figure 1). A 5th metatarsal avulsion fracture causes localized pain, swelling, and difficulty walking. During an avulsion injury, a variable size fragment of bone at the base of the 5th metatarsal is pulled off by a strong plantar ligament and the peroneus brevis tendon that is attached to this part of the bone. In most instances, this type of fracture can be treated non-operatively, with relative immobilization in a walking boot combined with limited weight-bearing. This type of injury needs to be differentiated from a “Jones fracture“, which occurs slightly further towards the center of the 5th metatarsal. Some clinicians refer to 5th metatarsal avulsion fracture as a “Pseudo Fracture” or a “Dancer’s Fracture.” However, more commonly a “Dancer’s fracture” is considered a spiral fracture of the 5th metatarsal shaft that was originally described in Dancer’s.

Clinical Presentation
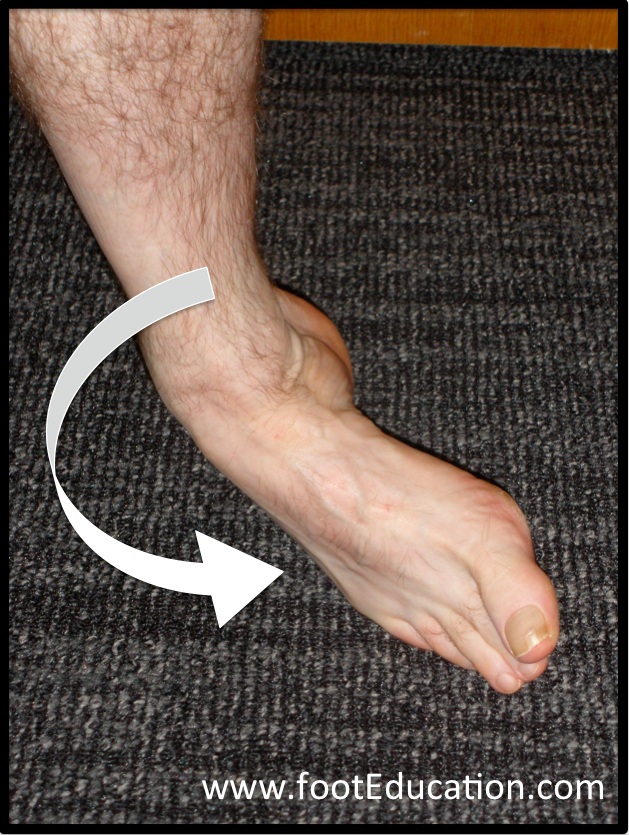
A patient who suffers an acute rolling of their ankle can also injure the base of the 5th metatarsal (See Figure 1). This will produce immediate pain over the outside aspect of the foot. It can be associated with significant swelling. Difficulty with balance due to weakness of the peroneus brevis also occurs. Over time, the skin can turn black and blue. This injury will be associated with quite specific local tenderness over the base of the bone, on the outside of the foot (the 5th metatarsal). Patients who have suffered a 5th metatarsal base avulsion fracture will give a history of a twisting injury to their ankle and foot (inversion plantarflexion injury), similar to what occurs with an ankle or foot sprain (Figure 2). The fracture commonly occurs in middle-aged or older women with low bone density (osteopenia or osteoporosis).
Physical Examination
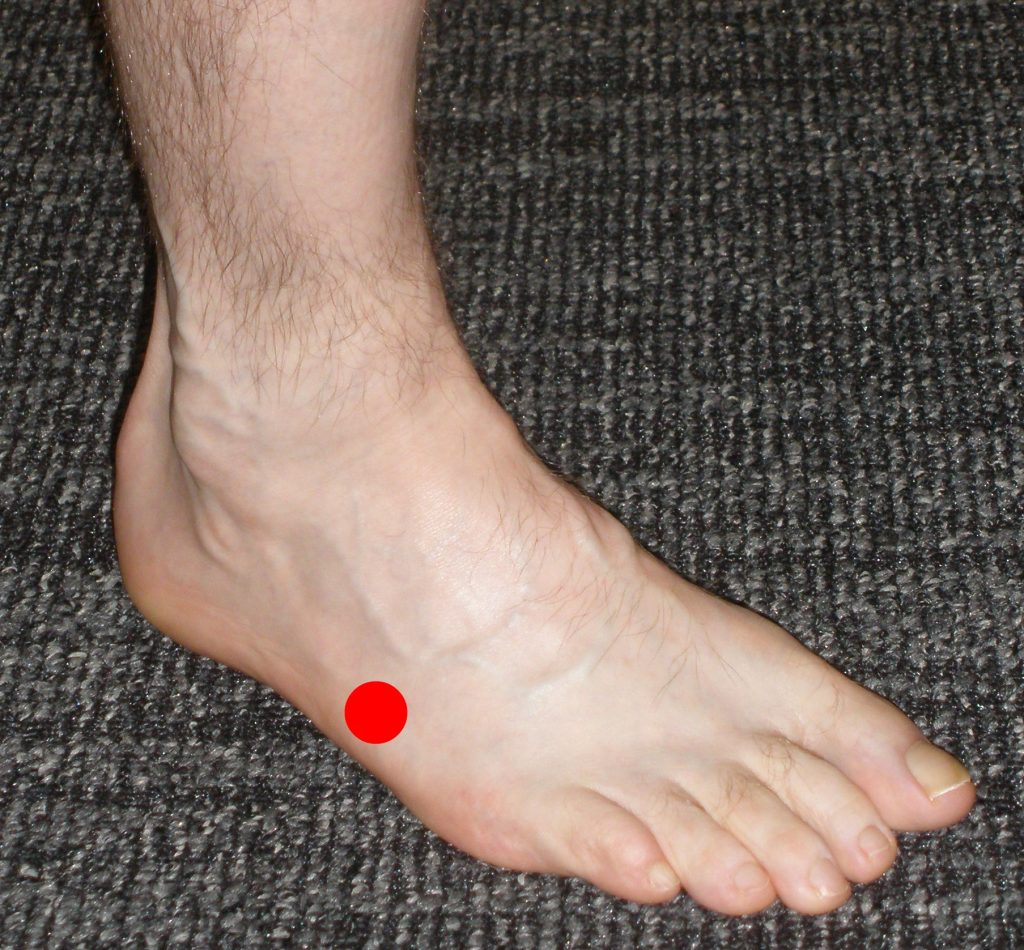
When pressing on the outside of the foot, there will be marked tenderness at the base of 5th metatarsal (Figure 3). There may be tenderness over a large area of the outside of the foot. However, the main tenderness will be at the base of the 5th metatarsal. On exam, it is determined if the patient can still move their foot to the outside (eversion of the foot). This is done by placing the foot in an everted position and asking them to maintain that position against some resistance. This assesses for continuity of the tendons that evert the foot. Doing this usually creates some discomfort for the patient. However, they usually are able to perform the action though with decreased strength compared with the opposite side.
Imaging Studies
X-ray of the foot will reveal an avulsion (“pulling off”) fracture of the base of the 5th metatarsal. The size and displacement of the fractured fragment may vary considerably. There will be more gapping at the fracture site, plantarly (on the bottom of the foot) and on the outside of the bone (lateral side), compared to the inside of the bone (medial side – Figures 4A and 4B).


Treatment of 5th Metatarsal Avulsion Fractures
A 5th metatarsal avulsion fracture is an injury that can usually be treated non-operatively. If the patient has the ability to actively move the foot outwards (eversion), the injury will likely heal with non-operative treatment. Treatment involves relative rest and time to allow the fracture to heal. Typically, patients are placed in a walking boot to immobilize the peroneus brevis tendon. For the first few weeks, they will have to significantly limit their walking and may need crutches. As the swelling settles and the fracture starts to heal, patients can begin walking more extensively in the boot as comfort allows. Usually by 6 weeks, there is enough healing to allow them to transition to a stiff-soled shoe with lots of padding. This is a frustrating injury because it takes a long time for healing to occur. Patients are often still symptomatic 8 weeks or more after this injury. It can be many months before the bone is completely healed and a full recovery has been achieved.
Surgical Treatment of 5th Metatarsal Avulsion Fractures
Although uncommon, when there is complete displacement of the fracture fragments and union is unlikely, surgery may be indicated. In other circumstances, when a person’s employment or recreation require a reliable and routine return by 6 weeks, surgery may also be indicated. In these cases, the bone fragments are repositioned and stabilized with a screw and weight bearing may be started immediately.
It is important not to overlook other associated injuries such as an ankle sprain. Ankle or foot instability, when present should be addressed with physical therapy to avoid recurrence of ankle inversion injuries.
A 5th metatarsal avulsion fracture is often confused with a 5th metatarsal metadiaphyseal stress fracture (Jones fracture). A Jones fracture can occur as a result of repetitive loading to the area (a stress fracture) or acute trauma. Unlike a Dancer’s fracture, a Jones fracture will more commonly fail to heal without surgery despite extended periods of non weight bearing. A 5th metatarsal avulsion fracture may sometimes be referred to incorrectly as a pseudo-Jones fracture because of the resemblance to a Jones fracture and the common mechanism of injury.
Click Here for a Summary Handout about 5th Metatarsal Avulsion Fractures
Edited by Stephen Pinney MD, February 17th 2026. Previously Edited by David N. Garras, MD and Lance Silverman, MD