
Calcaneus Fractures
Heel Fracture
Summary
Watch Video: Calcaneal Fracture
Patient Handout: Calcaneal Fractures
A typical depressed calcaneal fracture (Figure 1) is perhaps the most serious common foot injury. Depressed (crushed) calcaneal fractures occur when the heel is directly or indirectly loaded with excessive force, such as in a fall from a height or in a motor vehicle accident where the heel may be driven into the floorboard. There are both non-operative and operative treatments available for this injury. Operative treatment allows for the bone fragments to be repositioned so that they can heal in an improved position (it does not speed bone healing which usually takes 8-12 weeks). However, surgery requires a high degree of skill and experience on the part of the surgeon. Surgical complications such as wound breakdown or deep infection are not uncommon, and can be extremely serious. Complications are higher in patients who are smokers, diabetics, have vascular disease, or who have excessive swelling. The long-term prognosis is somewhat guarded with both operative treatment and non-operative treatment, with some hindfoot stiffness and pain being common. Arthritis is common due to the injury itself and risk of subtalar arthritis or chronic pain may not improve following surgery.
Figure 1A: X-ray of foot showing a normal calcaneus from the side

Figure 1B: X-ray of a calcaneus fracture

Clinical Presentation
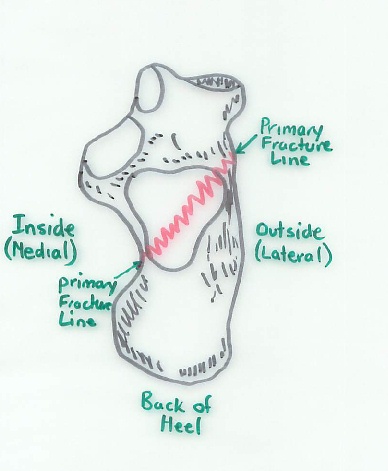
Patients who have suffered a calcaneus (or heel bone) fracture present with acute pain and a large amount of swelling over the heel. They are usually unable to bear weight on the involved foot. The fracture itself occurs when the lower bone of the ankle (talus) gets driven into the upper part of the heel bone (calcaneus). This causes the calcaneus to break (Figure 2). People often break their calcaneus when they fall from a height onto their feet. The calcaneal bone is somewhat analogous to a complicated shaped egg. It has a hard shell (cortical bone) on the outside, and very soft cancellous bone on the inside. When it breaks, there is a primary fracture line running from the inside distal part of the calcaneus to the outside hind part of the calcaneus (Figure 3).
Figure 2A: Mechanism of Typical Calcaneal fracture – Side view
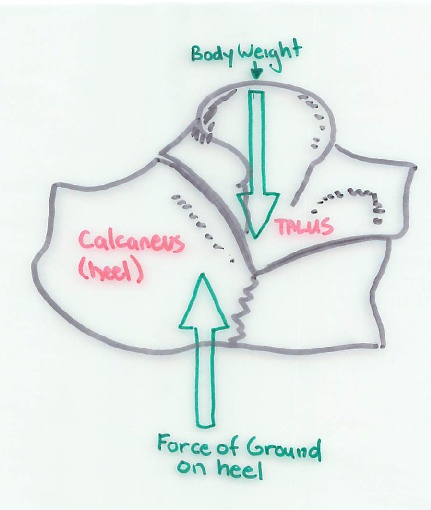
Figure 2B: Mechanism of Typical Calcaneal fracture – Viewed from the back
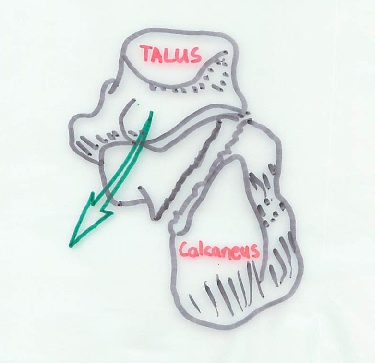
Figure 3: Primary Fracture line viewed from the top (also showing secondary fracture lines)
In addition, there is often a series of other fracture lines. The calcaneus, in many ways, breaks the same way as an egg would break into a number of different pieces. The fracture pattern will vary for each patient and injury.
Physical Examination Related to Calcaneal Fractures
In patients with calcaneus fractures the physical examination usually demonstrates tremendous swelling around the involved heel. In some patients, there will be a break in the skin, representing an open fracture. Open fractures constitute an orthopedic emergency. Usually, the sensation in the foot is intact. In addition, blood supply to the foot is usually intact, although this does need to be assessed following the injury. It is also common to have other injuries, such as a fracture involving the ankle or another part of the foot. A lumbar (lower) spine fracture will occur in about 10% of patients who suffer a calcaneal fracture. This is a fracture in the lower to mid back which essentially crushes one of the vertebras. The same mechanism that produces a calcaneal fracture will predispose a patient to having a lumbar burst fracture.
Calcaneal Tuber Fracture
The Achilles tendon attaches to the back portion of the calcaneus. Injuries were the Achilles tendon pulls off a piece of bone (avulsion fracture) can lead to soft tissue injury and are an orthopaedic emergency as skin death (necrosis) can occur rapidly. These injuries require immediate intervention usually.
The peroneal tendons on the outside of the ankle can occasionally dislocate in addition to a calcaneus fracture. The treating provider will examine the patient for this. Dislocated peroneal tendons are usually treated surgically when they occur with a calcaneus fracture.
Imaging Studies
X-rays are helpful when a calcaneal fracture is suspected. Typically, a lateral x-ray demonstrating the foot from the side (Figure 4), as well as an axillary heel view (Harris view) showing an end-on view of the heel are taken. This allows the basic fracture pattern to be identified.
Figure 4: X-ray of fractured calcaneus from the side

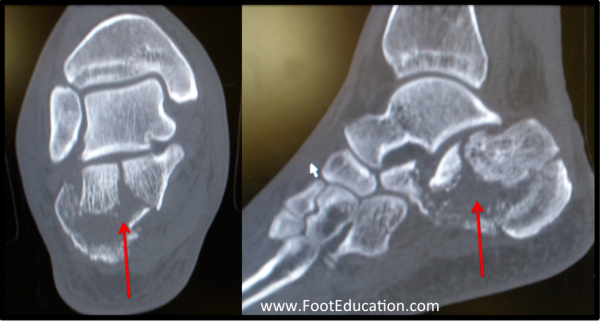
To more thoroughly understand the fracture pattern, particularly if surgery is a possibility, a CT scan will be ordered (Figure 5). On the CT scan, the number of fracture lines extending through the posterior facet of the calcaneus, which forms a mobile joint with the talus (subtalar joint), is important. The more fracture lines extending through this area of the subtalar joint the greater the likelihood of significant post-traumatic arthritis.
Figure 5: CT scan of a fractured calcaneus
Treatment of Calcaneus Fractures
Non-Operative Treatment
Calcaneal fractures can be quite difficult to treat, and the recovery can be prolonged. It is not uncommon and, in fact, may be the norm to have some element of post-traumatic subtalar arthritis as a result of this injury.
Non-operative management of calcaneal fractures does not mean NO treatment. Non-operative management includes a prolonged period of non-weight bearing to allow the fracture to heal. This typically needs 10-12 weeks to allow the calcaneal fracture to heal enough to bear full weight. During that time, the patient is treated with appropriate pain control. This includes elevation to limit swelling, ice to decrease the swelling and improve local symptoms, and pain medication. Patients may be treated in a splint, cast, or walker boot based on treating doctor’s preference for the injury along with other factors.
An important active part of non-operative management is early work to optimize range of motion. These exercises are often as simple as drawing out a figure-of-eight with the big toe, as well as using a towel over the toes to bring the foot up towards the shin (dorsiflexing the ankle).
Large studies have suggested that results of non-operative treatment are only marginally worse than the results of operative treatment, when all the patients are considered. If a patient is at high-risk of operative complication, non-operative treatment should be employed as the risks of operative treatment for this injury can be quite severe. Patients who smoke, are diabetic, have vascular disease, have an active Worker’s compensation claim, or are older, are thought to have a higher risk of complications and/or poor outcome with surgery.
Operative Treatment
Operative treatment involves reconstructing the calcaneus in order to return its pre-injury shape and restore the subtalar joint surface, which is on the top part of the calcaneus and allows side to side motion of the foot. Surgery is designed to increase long term function and decrease the risk of arthritis in the future. For each patient, this treatment needs to be individualized. It is important that the surgeon involved has experience with these types of fractures. Operating through excessively swollen tissue has been shown to significantly increase the risk of wound healing problems and infection. For this reason, it is often standard practice to wait until the soft-tissues swelling has settled, which can be 10-14 or more days after the injury. The worst results of calcaneal fracture treatment occur when an operatively treated fracture is complicated by a bad, deep infection or a significant wound breakdown. It is not unheard of in these situations that a patient will eventually require an amputation.
Extensile Approach to Surgical Treatment of Calcaneal Fractures
Operative treatment is usually performed through an “extensile” incision on the outside of the heel. The fracture fragments of the calcaneus are systematically reduced back into their original position. If they cannot be anatomically reduced, this will significantly reduce the effectiveness of the surgery, often to the point where non-operative management should be undertaken. After the bones have been repositioned, they are fixated with a combination of screws and plates (Figure 6). The fixation is customized depending upon the fracture pattern.
Figure 6: Calcaneus following surgical fixation

Sinus Tarsi Approach to Treatment of Calcaneal Fractures
For some patients, some surgeons will elect to fix the fracture through a smaller incision on the outside of the ankle. This “sinus tarsi” approach has a lower wound complication rate compared to a traditional “extensile” approach that exposes the entire outside (lateral) part of the heel (calcaneus) bone. However, it can be difficult or impossible to fully correct the position of the calcaneus fracture and associated injury to the subtalar joint with this smaller “mini” approach. For this smaller approach to be effective the surgeon must be quite experienced and the fracture pattern must be such that it is amenable to this type of surgical treatment.
Percutaneous Treatment of Calcaneal Fractures
With certain fracture patterns, it may be possible to perform a percutaneous procedure. Percutaneous treatment (operating without making a large incision) involves skewering part of the fracture with a straight wire (K-wire), and manipulating it into an improved position. This is done through a few stab incisions. Unfortunately, less than 10% of the calcaneal fractures fit into this category, and most require an open procedure if the bone fragments are to be adequately repositioned (reduced).
Figure 7: Calcaneus following percutaneous repair

Following surgery, the recovery time is similar to that for non-operative treatment. Essentially, the patient needs 10-12 weeks of non-weight bearing to allow the fracture to heal.
Surgical Complications
Complications of operative treatment are not uncommon. The major complications include:
- Deep wound infection: Because of the tenuous skin over the outside of the heel, a wound infection often extends down to the bone potentially leading to osteomyelitis (bone infection).
- Wound healing can be an issue because the soft-tissue on the outside of the heel has a tenuous blood supply.
- Sural Neuritis: The sural nerve, which innervates the outside of the foot, is often stretched or injured in the surgical approach, and can become scarred or injured in the course of the surgery.
- Nonunion of the calcaneus is possible, although it is uncommon.
- Subtalar arthritis is not so much a complication as it is a common long-term effect of the injury, leading to pain and stiffness in the hindfoot. This will manifest itself with symptoms when the patient stands for a prolonged period of time, or walks on uneven ground. This could be a problematic symptom for patients that are on their feet a lot. For these patients, it may even be necessary to eventually perform a primary subtalar fusion.
- Deep Vein Thrombosis (DVT)
- Pulmonary Embolism
Patient Handout: Calcaneal Fractures
Edited by Stephen Pinney MD June 17th, 2025. Previously edited by Marcus Coe, MD and Michael Shereff, MD