
Stubbed Great Toe
Summary
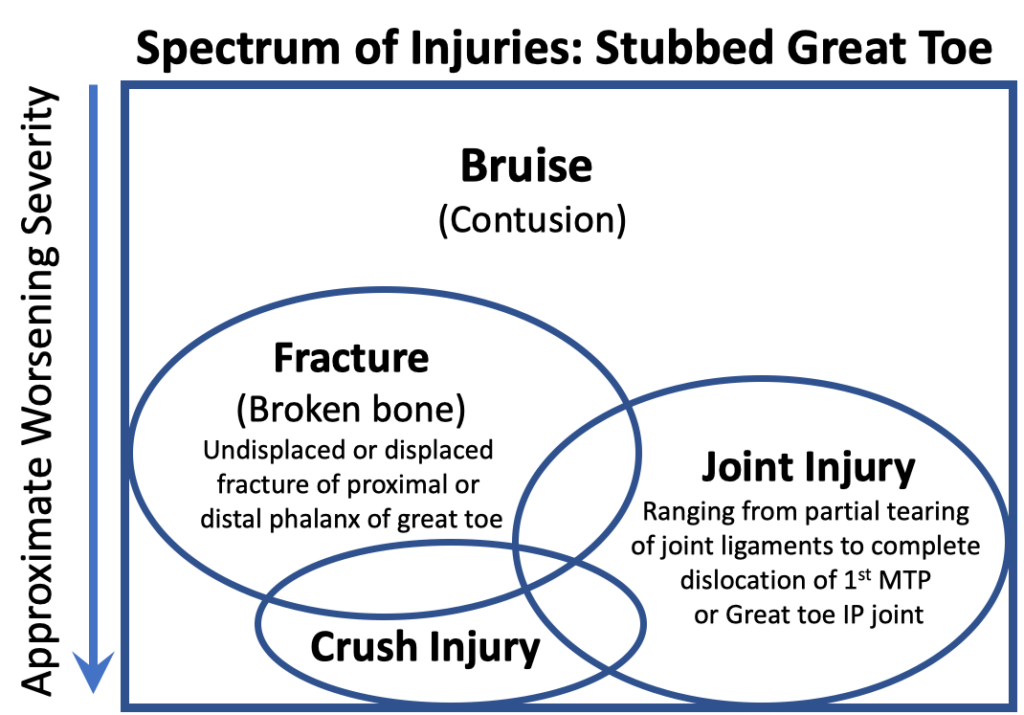
Stubbing the great toe by accidentally smashing it against a solid object is unfortunately a relatively common injury. This type of great toe injury is painful and frustrating! The extent of injury to the great toe varies widely from local bruising with no structural damage to a major injury with fracturing of the bones and potential disruption of one or more of the great toe joints. Fortunately, the vast majority of stubbed great toes, while initially quite painful, do not create significant disruption of bones or soft tissues. These types of stubbed great toe injuries can be treated conservatively. However, if there is a notable new deformity of the great toe; a laceration or disruption of the soft tissue suggesting that the bones and deeper structures have come through the skin; or the patient has diabetes or other medical conditions that may affect the blood supply to the great toe the patient should seek an assessment and care by a physician. The spectrum of injuries that can be associated with a stubbed great toe are outlined in Figure 1 and described below.
The Spectrum of Injuries Associated with a Stubbed Great Toe
There are a variety of different injuries that can occur from a stubbed great toe (Figure 1). These include:
- Great Toe Bruise – Contusion
- Joint Injury from a Stubbed Great Toe
- Great Toe (Phalangeal) Fracture
- Great Toe Crush Injury
Great Toe Bruise – Contusion
A contusion or bruise of the great toe is the most common injury resulting from a “stubbed” great toe. It occurs when a direct blow to the toe causes bruising but no appreciable injury to the joint capsule, joints, or bones. Bruising is essentially damage to the soft tissues leading to bleeding in the soft tissues. This is also referred to as a contusion. Although a great toe contusion will usually resolve uneventfully, the injury can be very painful — especially at the time of the injury.
Treatment of a bruised great toe involves relatively protecting the toe by: limiting activities; wearing a protective stiff shoe with a wide toebox to prevent further injury; and occasionally taking an anti-inflammatory medication. Icing can help limit the pain and decrease the swelling in the short term. A bad bruise following a stubbed great toe will usually resolve uneventfully, although it can be a week or more before symptoms have settled. Some persistent stiffness of the joints of the great toe has been known to occur. Additionally, it can often be difficult to differentiate between a painful bruise and a more involved injury such as a fracture of one of the bones of the great toe, or an injury to the ligaments of one of the joints.
Joint Injury from a Stubbed Great Toe
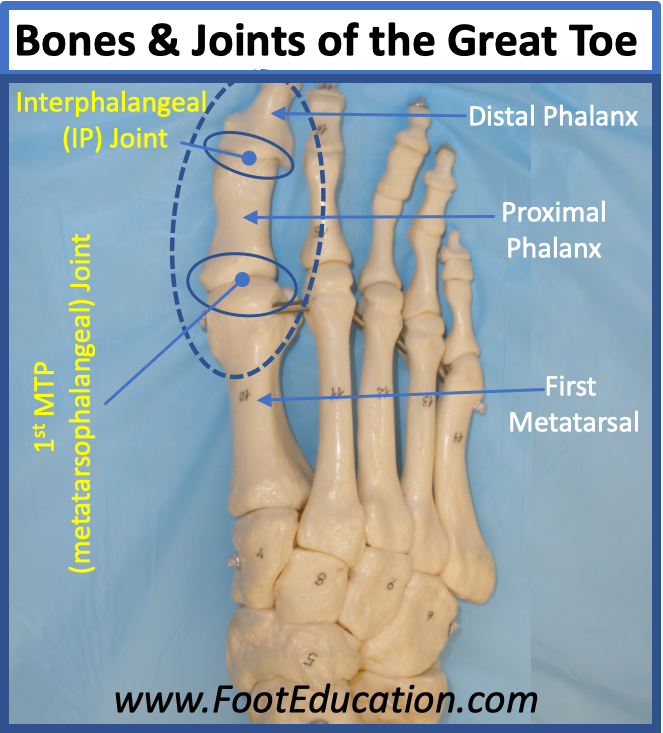
Smashing the great toe against a solid object will create bruising, and if severe enough will cause an injury to one or both of the joints associated with the great toe. These joints include the interphalangeal joint and the first metatarsophalangeal joint (Figure 2). The specific joint injury may include: tearing of the ligaments that stabilize the joint: damage to the joint cartilage; or even a fracture that extends into the joint. The joint injury can range from mild partial tearing of some of the fibers of one of the joint ligaments to a severe fracture dislocation of the joint with complete disruption of the joint ligaments, extensive damage to the cartilage, and a displaced fracture that extends into the joint. The appropriate treatment and the expected recovery time will be dictated by the extent of the joint injury as well as the primary joint that is affected. It should be noted that a turf toe is a special type of great toe joint injury. It occurs when the great toe is forced upwards (dorsiflexed) and the strong soft tissue stabilizing the lower part of the joint (the plantar plate) is partially or completely disrupted. For more details on this injury, check out our turf toe page.
Treatment of a stubbed great toe with an associated joint injury can be divided into: 1) acute and 2) definitive management.
Acute treatment of a stubbed toe focuses on pain control, limiting swelling, and ensuring that any injured joint is appropriately positioned including reducing any joint dislocations. Clinical examination and, if necessary, x-rays will determine if any of the joints are dislocated or subluxed (i.e. malpositioned) and identify any significant fractures that are present. A dislocated great toe joint following a direct blow is uncommon. However, if one of the joints is dislocated or significantly out of position, it will need to be reduced under anesthesia by an appropriately trained physician. Fortunately, while swelling and pain is normal after stubbing the great toe frank displacement of one of the joints is relatively uncommon.
Acute management of a stubbed great toe with a joint injury includes: limiting activities; elevating the foot to limit swelling; icing the injured area; protecting the toe with a stiff soled shoe with a wide toebox; and using crutches or a cane if necessary. This acute treatment may need to be continued for a few days, a week, or even longer depending on the extent of the injury. However, eventually the swelling and pain will settle.
Definitive management of a stubbed great toe with a joint injury is dictated by the nature of the injury. Fortunately, most of these injuries, although severe, can be managed without surgery. However, if the injured joint is malpositioned, or there is a significantly displaced intra-articular fracture then surgery may need to be considered. Once the toe is in an acceptable position, treatment involves protecting the toe for a number of weeks while the bones, ligaments, and soft tissues heal. This is done with a stiff soled shoe or boot with lots of space around the toe to allow for swelling. It can often take 4-6 weeks or longer for the tissues to heal. During that time the injured joint will often become quite stiff, necessitating some mobilization exercises once a graduated return to activity has been started. Some residual joint stiffness following a bad stubbed great toe injury is not uncommon.
Great Toe (Phalangeal) Fracture
A stubbed great toe will often lead to a fracture of one or both of the bones of the great toes (the proximal and distal phalanx). However, the extent of the fracture can vary widely. Many fractures are essentially undisplaced. They appear as mere cracks in the bone. Other fractures are angulated or partially displaced but still in acceptable position. A few fractures are completely displaced or market angulated and these fractures will need to be repositioned either with a manipulation of the bones under local anesthetic or with a formal surgical operation. Fortunately, the vast majority of stubbed great toes, even those with fractures, do not require repositioning or surgery. Furthermore, there are a variety of different fracture patterns that can occur. Many are undisplaced with a simple crack through the bone that can be identified on x-ray. Another common fracture is an avulsion fracture, whereby the strong ligaments of one of the joints pulls off a fragment of bone where the ligament attaches to the bone usually not with excessive displacement. Less commonly, fractures of the great toe may be significantly displaced or angulated. It is these less common displaced fractures that may need definitive treatment such as repositioning or surgery. Additionally, fractures that extend into one of the great toe joints and lead to notable malposition of the joint will also often need to be fixed surgically. Surgery to fix an angulated, displaced, or intra-articular fracture involves repositioning the fracture fragments and then stabilizing reduced fracture with screws and possibly a plate.
If the great toe fracture or fracture is deemed to be in an acceptable position or the fracture has been corrected surgically, the recovery is usually straightforward. Although, the ultimate recovery can take many months. There is an initial period of about six weeks where the toe is relatively immobilized with a stiff soled shoe. Patients are encouraged to elevate their foot to limit swelling. Walking for limited distance through the heel may be allowed. However, activity during this time will usually be minimal. Once the bone and soft tissues have adequately healed mobilization exercises to regain motion in the affected joints can be aggressively pursued. However, some residual stiffness in these joints is common following this type of injury.
Edited by Stephen Pinney MD February 20th 2026.