
Lisfranc Injury (Midfoot Sprain)
Edited by
Summary
Watch Video: Lisfranc Injury
A Lisfranc injury is a significant injury that involves the midfoot. It is sometimes referred to as a midfoot sprain and it is often has a lengthy recovery time -especially compared to the average ankle sprain. A Lisfranc injury can involve any combination of fracture, joint dislocation, and/or injury to the stabilizing joint ligaments. The injured area is the junction between the midfoot and the forefoot (tarsometatarsal joint -Figure 1A). It is named after the 19th century French surgeon Jaques LisFranc de St. Martin who described an amputation through the foot where this injury happens. The classic story told is that this injury was seen when soldiers were knocked off of their horses with their feet caught in the stirrup. Significant disruption of these midfoot ligaments (Figure 1), especially with additional breaking of the midfoot bones, can lead to pain, swelling, and inability to weight-bear. During normal standing and walking, the ligaments of the midfoot experience forces that are 2-3 times body weight. These ligaments and bones must heal before normal walking can occur. This often takes many months. A stable injury to the midfoot, whereby these ligaments are injured (perhaps stretched or only partially torn) can be treated without surgery. This involves 6 weeks or more of non-weight-bearing or limited weight bearing followed by a physical therapy program to regain full function. A displaced Lisfranc injury usually requires surgery to stabilize the injury followed by an extended period of recovery.
Figure 1A: Lisfranc Joint
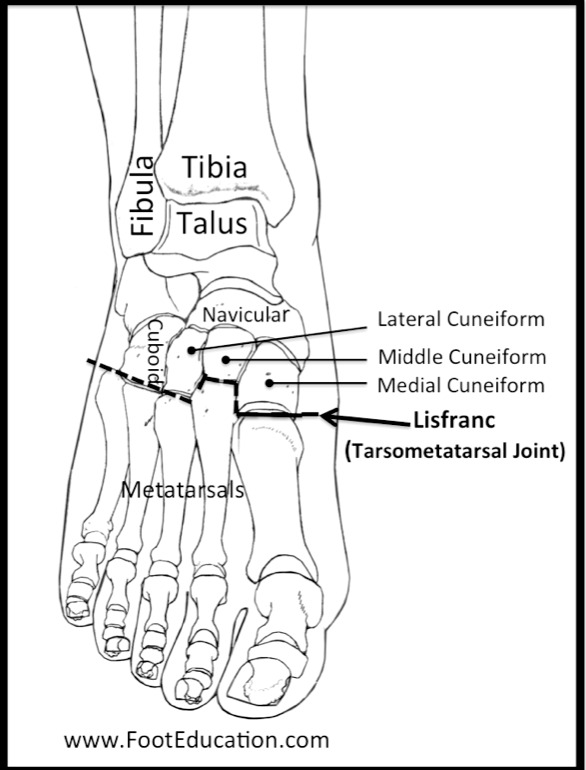
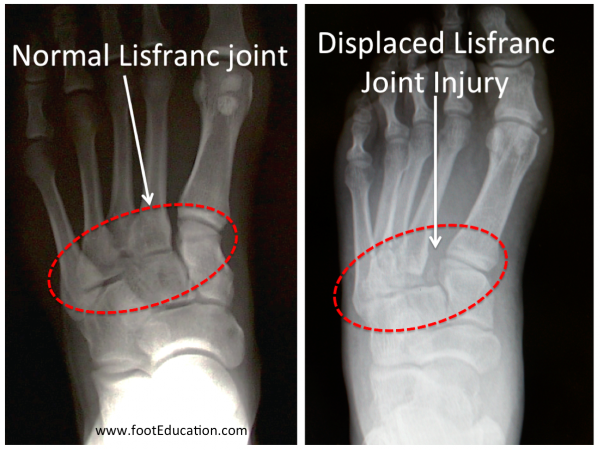
Figure 1B: Lisfranc Fracture
Printable handout
Clinical Presentation
Lisfranc injuries typically occur when the foot is twisted under the load of body weight (ex. trip off a curb) or by another person (sports) or thing (car accident). When this happens, the strong midfoot ligaments may partially or completely tear and sometimes the bones will break (Figure 1A and 1B). This can occur via a number of mechanisms including:Clinical Presentation
- A twisting injury such as often occurs in sporting activities (ex. football), where the toes are planted on the ground and the heel is loaded.
- A slip and twist to the foot while stepping off a curb.
- Impact of the foot on the brake pedal, such as occurs in a motor vehicle crash.
Patients with Lisfranc injuries usually have significant swelling and pain in the middle part of the foot (Figure 2), and often have bruising on the bottom of the foot (Figure 3). It is usually very difficult or impossible to put weight on the injured foot or leg due to pain. Lisfranc-type injuries range from mild sprains with a stable foot to complete tearing of the ligaments of the midfoot along with fractures of multiple midfoot bones. Because the ankle is often not part of the injury, this problem may be minimized as “just a foot sprain.” However, a Lisfranc injury (midfoot sprain), even one that is not displaced, is a serious injury. Providers need to be thinking about this injury so it can be diagnosed and treated in a timely manner to obtain the best result.
Physical Examination
In patients who have suffered a Lisfranc injury physical examination reveals specific tenderness to palpation across the midfoot region (Figure 2). There will often be significant swelling of the foot. Patients with Lisfranc injuries will not want to bear weight on the injured foot. In addition, manipulation of the bones of the midfoot, specifically twisting he foot downwards and to the outside (pronation and abduction of the forefoot), will create pain. Bruising in the center bottom aspect (plantar) of the foot (Figure 3) is common and should raise suspicion for a significant injury.
Figure 2: Location of Pain
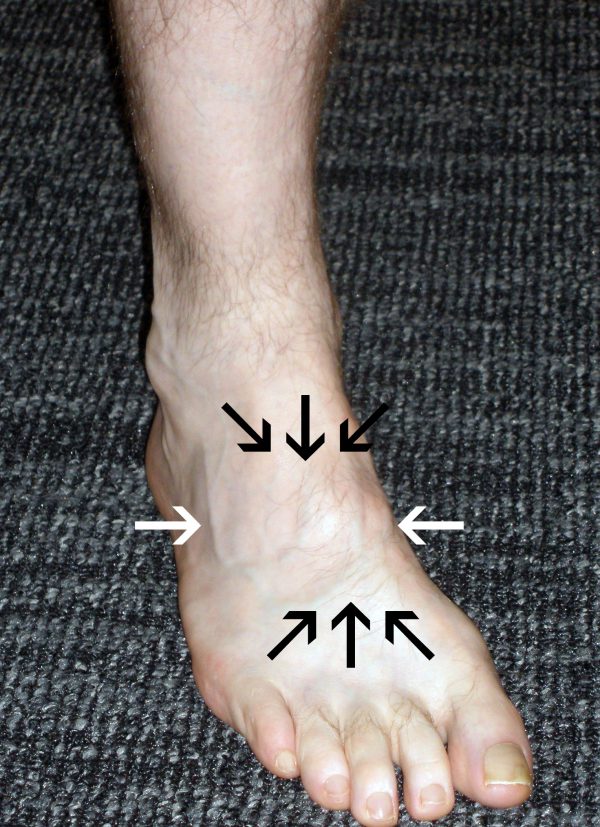
Figure 3: Bruising from Lisfranc Injury

Imaging Studies
X-rays are taken to identify whether the injury is displaced or non-displaced. Weight-bearing foot x-rays are helpful to determine if the midfoot injury is stable (sprain) or unstable (Lisfranc). Obtaining a comparison film of the other foot is helpful to see the normal alignment of the person’s foot (which can vary from person to person). A CT scan or MRI may be necessary if the diagnosis or the extent of the injury is unclear. These tests help to see the small bony detail in this region of the foot, as well as hard to see fractures and joint displacements. Occasionally, it may be necessary to perform stress x-rays (obtaining an x-ray while twisting the foot) to determine if the foot is stable or unstable.
Classification
There are several classification systems for Lisfranc injuries, however the crucial determination is whether or not the injury is “stable” or “unstable”. in a stable Lisfranc injury the ligaments of the midfoot are partially torn, but still stable, so the bones of the midfoot remain in a normal position even when loaded. In an “unstable”Lisfranc injury there is a disruption of one or more of the ligaments of the midfoot (usually including the Lisfranc ligament) that leads some of the bones of the foot to become displaced, either partially (joint subluxation) or completely (joint dislocation).
Treatment
Stable Lisfranc injuries are usually treated without surgery. Treatment involves protecting the injured foot in either a cast or a prefabricated boot. Patients often need at least a 6-week period where they are either non-weight bearing or minimally-weight bearing in order to facilitate healing of the injured ligaments and bones. In a stable injury, the midfoot ligaments are strained but still intact, so once an adequate amount of healing has occurred, patients can increase their activity level. Physical therapy to strengthen muscles and improve range of motion is often helpful in the recovery process. Even with a non-displaced “stable” injury that is consistent with “just a midfoot sprain”, full recovery can still take many months.
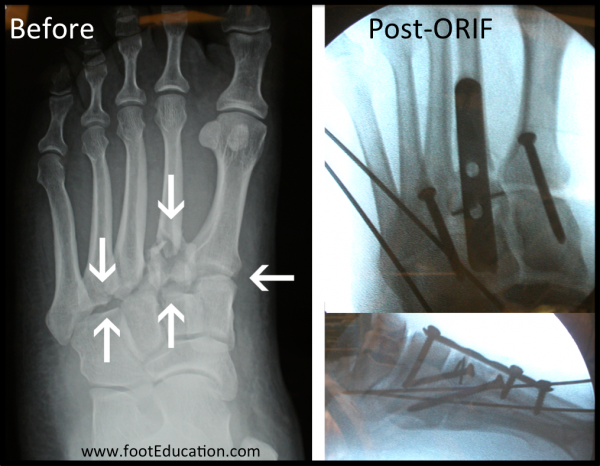
Displaced or Unstable Lisfranc injuries are usually treated surgically. Surgery is performed to restore joint alignment and stabilize the joint(s) with screws, pins, and sometimes plates (Figure 4). This allows the bones and the ligaments to be put back in their proper positions and held in place. This gives the ligaments a chance to heal. In some cases, it is necessary to fuse the involved joints (connect the two bones forever by getting them to heal together as one bone), eliminating the motion altogether. Many of these procedures will involve a second surgery to remove the hardware once the injury has healed. Recovery requires an initial period (often 6-8 weeks) to allow the bones and ligaments around the surgical area to heal. This is then followed by a rehabilitation program to regain lost strength, mobilize the soft-tissues, and regain motion in the joints of the foot. Complete recovery can take a year or more following a displaced Lisfranc injury.
Figure 4: Surgical Treatment of Lisfranc Injury
Recovery from Surgery
Recovery from Lisfranc injuries are lengthy because the midfoot sees tremendous stress during regular standing and walking. Post surgical treatment and recovery efforts depend upon the nature of the initial injury, what type of surgery is performed, and the surgeon’s preference. For a major Lisfranc injury, a typical recovery plan would include:
- 2 to 3 week period of splinted non-weight bearing, until swelling and discomfort settle down, and, if surgery was required, sutures can be removed.
- 6- to 8-week period of slowly increasing weight bearing in a specialized brace or cast.
- Gradual transition to weight bearing as tolerated in a specialized walking boot for an additional 4-8 weeks.
- Wean from the boot to a stiff sole shoe at 10-14 weeks from surgery, perhaps with subsequent use of a custom arch support or shoe insert.
A displaced injury takes many months of recovery. The majority of the recovery occurs in the first 6 months, but it is often a year or more before patients reach their point of maximal improvement.
If the surgical treatment fails or the joint damage from the injury leads to severe arthritis, then a fusion (arthrodesis) of the Lisfranc joints may be necessary. Despite the stiffness of a fused joint, most patients with successful fusion of the midfoot joints have good function of the foot.
Printable handout
Edited on July 13th 2025 by Stephen Pinney MD. Previously edited by Daniel Farber, MD and Christopher DiGiovanni, MD