
Fibular Avulsion Fracture
Summary
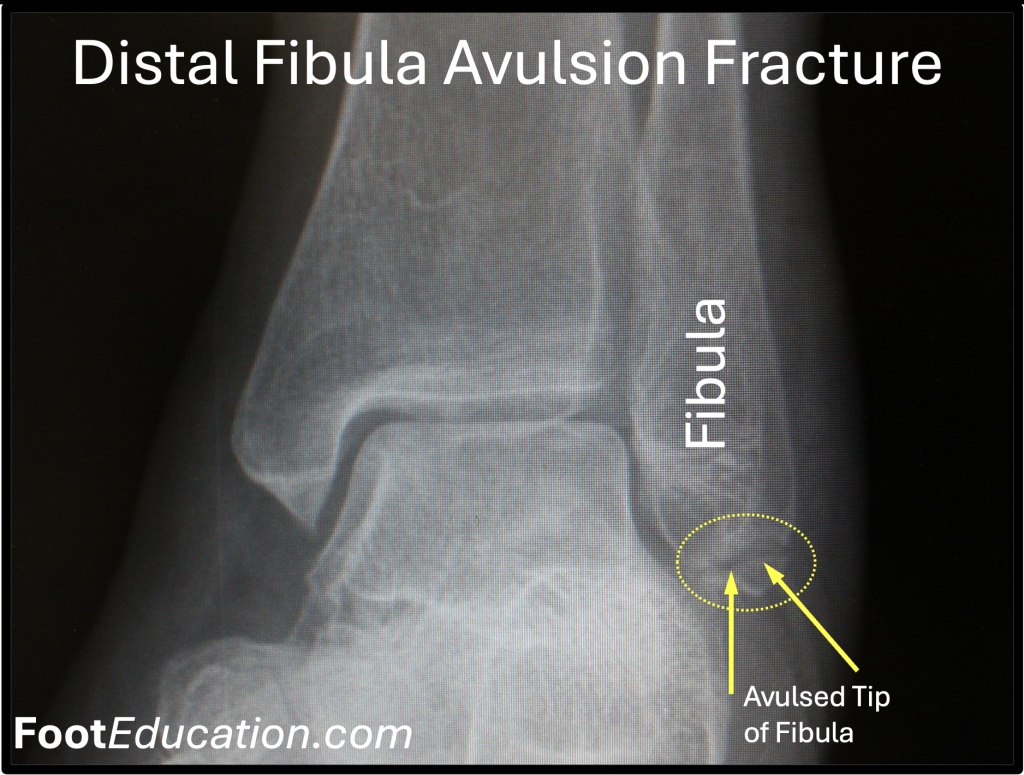
Fibular avulsion fractures most commonly occur from an inversion of the ankle that causes the ankle ligaments to pull a small piece of bone off of the end of the fibula. The injury produces pain, tenderness, and swelling of the ankle making weight-bearing difficult or impossible. The diagnosis is made by x-raying the ankle (Figure 1). The fracture is treated by immobilizing the ankle with a boot or ankle brace with gradual reintroduction of weight bearing over a period of weeks. Surgery is rarely indicated. Although a fibular avulsion fracture is technically an “ankle fracture” the injury is essentially the equivalent of a moderate-severe ankle sprain and should not be mistaken for a more severe ankle fracture which often does require surgery.
Clinical Presentation
Fibular avulsion fractures are usually the result of an acute inversion injury to the ankle. The injury is essentially a moderate-severe ankle sprain except that in addition to tearing the outer (lateral) ankle ligaments a small fragment of the prominent outer ankle bone (fibula) is pulled off (avulsed) by the attached ligament. The sudden inward rolling (inversion) of the ankle places excessive strain on the outer ankle ligaments attaching the fibula to various bones in the ankle (talus and calcaneus). As a result, the ligaments tear or in some instances a section of the ligament may stay intake and pull off (avulse) a small piece of bone from the end of the fibula. Typically, the avulsed fragment of bone is small and does not enter the ankle joint as it is still attached to the ligament that pulled it off the bone.
The highest prevalence of fibular avulsion fractures occurs in elderly females and young adult males. Elderly females often have osteoporosis leading to weakening of the bone whereas young males often have very strong ligaments. In both situations the ligament ends up being stronger than the fibular bone that it is attached to leading to failure through the bone.
Physical Exam
The injury will present similarly to an ankle sprain with swelling and tenderness around the outside bony prominence of the ankle (lateral malleolus). The injury can be quite painful making weight-bearing on the ankle very difficult, but not always impossible.
Imaging Studies
A simple set of ankle x-ray from the front and from the side (AP and lateral views) is sufficient to make the diagnosis of fibular avulsion fracture. Both x-ray views are necessary as the fracture may only be visible in one projection.
Treatment
Small fibular avulsion fractures can be treated the same as a severe ankle sprain. Rest, ice, elevation, and anti-inflammatory medication can be helpful in the first few days after the injury. Immobilization in a cast or splint is common immediately after the initial injury. The patient can be transitioned to a walker boot, or ankle brace in the following 1-2 weeks. It is helpful to work on very gentle range of motion exercises as the ankle swelling begins to settle. After 2-6 weeks the symptoms will usually have settled to the point where patients can begin weight bearing on the ankle, either in a walker boot or an ankle brace. Once most of the acute swelling and pain has settled the patient will benefit from physical therapy to work on regaining strength, ankle motion, and balance. Surgery is rarely indicated for a small fibular avulsion fracture. In some patients a fibular avulsion fracture will be associated with, or lead to, ankle instability that may eventually benefit from surgery.
Edited by Stephen Pinney MD June 17th, 2025