
Dorsiflexing 1st Metatarsal Osteotomy
Indications
This type of procedure is indicated for patients with a high-arched foot, which can lead to a variety of critical problems, including recurring ankle sprains, ankle instability, peroneal tendonitis, 5th metatarsal stress fractures, and sesamoiditis. Usually, most conditions can be treated without surgery by either modifying activities, using various shoe inserts, and doing physical therapy exercises. However, surgical reconstruction, which may include a dorsiflexed osteotomy, may be beneficial for some patients where non-operative management has failed.
A common condition that leads to this type of surgery is Charcot-Marie Tooth disease, a condition where patients develop high-arched feet that can lead to significant symptoms. One of the main features of a high-arched foot is a plantarflexed first metatarsal, where the big toe is angled down more than the other toes. Therefore, this surgery is intended to correct the position of the first metatarsal. This surgery is often done in conjunction with other surgical procedures to fix a high arched foot.
Procedure
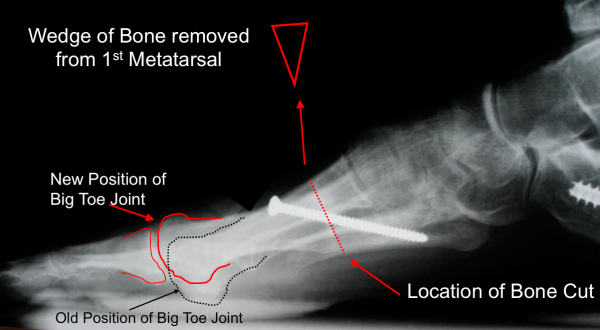
An incision is made over the top of the first metatarsal and dissected down to the bone. Once the top and side regions of the toe are exposed, a wedge of bone is removed. The toe is then repositioned upward to reduce the high-arch, and secured with screws, plates, or staples (Figure 1).
Figure 1: Removal of bone to reposition the big toe upwards and thereby alter the loading on the base of the big toe
Recovery
0-6 weeks Post-Surgery
Patients undergoing this type of surgery will typically need about 6 weeks for the bone to heal. During this period, the patient is either in a cast boot or in a post-operative shoe, and remains non-weight bearing or touch weight-bearing through the heel.
6 weeks + Post-Surgery
At 6 weeks postoperatively, if x-rays demonstrates satisfactory healing, patients are then allowed to begin weight-bearing in a Cam Walker or a stiff soled shoe, as tolerated.
Patients will gain approximately 75-80% of recovery in 4-5 months. However, it may take over a year to reach the point of maximal improvement.
Potential General Complications
Potential Specific Complications
Nonunion
A nonunion occurs when the fusion site fails to adequately fuse together. If a patient does have a nonunion or a delayed union, they may require a longer period of non weight-bearing, and in some instances will require revision surgery. The typical nonunion rate is about 5%. Risk factors include the surgical technique, the patient’s underlying condition, whether the patient smokes cigarettes, and the patient’s compliance with the postoperative non weight-bearing protocol.
Nerve Injury
Injury to the nerve on the outside aspect of the 1st metatarsal (deep peroneal nerve), or on the inside aspect of the first metatarsal (medial branch of the superficial peroneal nerve), can occur due to the placement of the incisions. Nerve injury can occur due to retraction, direct injury, or from scarring during the recovery process. If these nerves are injured or cut, the patient could end up with numbness or pain along the path of the nerve.
Over Correction/Under Correction
Determining the extent of correction required can be challenging for the surgeon. If the foot ends up in a less than an ideal position, the patient may end up with more symptoms and other conditions, such as metatarsalgia.
Painful hardware
Another potential complication with this procedure is having pain associated with the hardware used to secure the first metatarsal. It is not uncommon for patients to benefit from hardware removal after a dorsiflexing 1st metatarsal osteotomy, once the bone has healed.
Edited May 23, 2017
mf/ 11.19.18