
Attritional Plantar Plate Rupture – Chronic Plantar Plate Tear Associated with a Claw Toe Deformity
Background
An attritional rupture or stretching out of the plantar plate is often seen in conjunction with a claw toe deformity leading to forefoot pain (Figure 1). The rupture is considered attritional because it occurs due to repetitive loading and stretching overtime, rather than from a single traumatic episode. The metatarsophalangeal (MTP) joints are held in place by soft-tissues (ligamentous capsule) that surrounds the whole joint. The plantar plate is the thickened bottom part of this capsule. An attritional rupture of the plantar plate is often on the severe end of a spectrum of conditions that produce forefoot pain. The progression across this spectrum begins with basic metatarsalgia where there is increased loading over the forefoot causing localized discomfort and inflammation. However, the joint capsule and plantar plate remains intact -and there is minimal clawing of the toes. This can progress to more pronounced clawing of the toes with some looseness of the joint capsule. Eventually, there can be considerable attenuation or even rupture of the plantar plate. In its most severe form there may even be a dislocation of the affected toe. All of this occurs due to gradual repetitive overload of the forefoot during standing and walking combined with the development of a claw toe deformity. The load during these activities is usually disproportionately centered over the affected joint which contributes to the initiation and progression of symptoms.
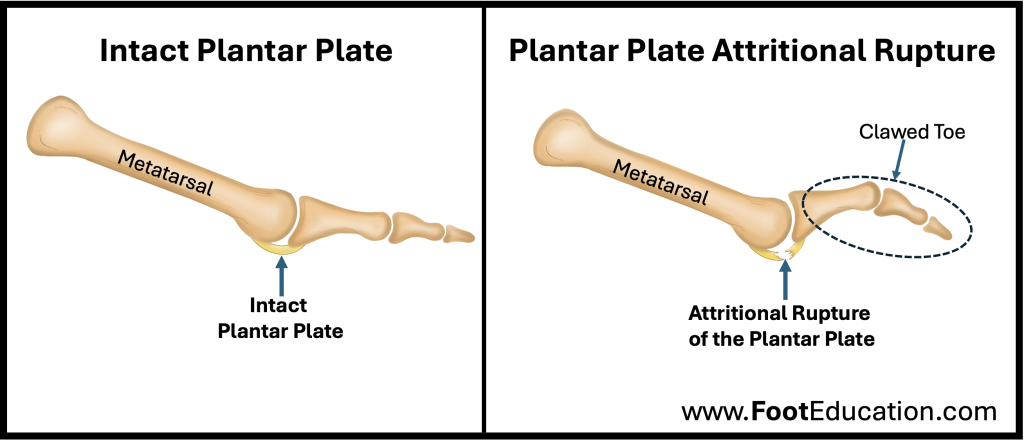
Figure 1: Plantar Plate Attritional Rupture
Signs and Symptoms of an Attritional Plantar Plate Rupture
Patient with an attritional rupture of the plantar plate will have localized forefoot pain, and usually pronounced clawing of the lesser toes. They will often complain that it feels like they are “walking on a marble” in the front of their shoe. This is because the metatarsal head at the base of the affected toe becomes quite prominent as the clawing of the toe increases and the plantar plate is stretched or torn. If there is obvious looseness or a dislocation at the base of the toe, the affected the plantar plate has likely been torn. However, in many instances, definitive tearing of the plantar plate is only identified on MRI or at the time of surgery.
Imaging Studies
Weight bearing x-rays of the foot will usually demonstrate maintenance of the associated joint space, although clawing of the toe may be noted. Additionally, often the associated metatarsal is long relative to the metatarsal bones on either side.
If an MRI is ordered it will often demonstrate attrition, partial, tearing, or complete disruption of the plantar plate. There may also be fluid in the associated MTP joint. Bone edema may be identified in the nearby metatarsal head. If there is dislocation of the associated toe this will be seen easily both on plain x-rays and on MRI.
Treatment
Non-Operative Treatment of an Attritional Rupture of the Plantar Plate
Attritional rupture of the plantar plate occurs in conjunction with an overload metatarsalgia and clawing of the lesser toes. Therefore, non-operative treatment is the same as it is for these conditions. Conservative treatment can often be quite successful, provided the associated MTP joint has not dislocated. Conservative treatment typically includes:
- Comfort shoes with a stiff sole and a rocker contour
- Soft orthotic insert can help disperse the forces more widely over the forefoot. These inserts usually do not need to be custom made
- Metatarsal pads can be very helpful when positioned correctly on the orthotic. Metatarsal pads help to offload the prominent metatarsal head.
- Activity modification to limit standing and walking often helps improve symptoms by reducing the repetitive loading through the painful forefoot.
- Taping or splints to reposition the affected lesser toe may be helpful for some patients.
Surgical Treatment of an Attritional Plantar Plate Rupture (with Metatarsalgia and a Claw Toe Deformity)
Surgical treatment is indicated for patients with claw toes and metatarsalgia who have failed conservative treatment -and patients who have severe deformities that are not amenable to conservative treatment. Many patients undergoing surgery to treat their metatarsalgia or claw toes will also be found to have a partially or completely torn plantar plate. In addition to the various surgical procedures used to address the metatarsalgia and clawing of the lesser toes consideration may be given to fixing a plantar plate rupture. However, it is still somewhat unclear, whether this extra plantar plate surgery is needed —or whether simply performing surgery to address the metatarsalgia and the associated claw toe will lead to a satisfactory result.
If the plantar plate is repaired or reconstructed, the surgery involves identifying the torn plantar plate and reattaching it to the base of the proximal phalanx with strong sutures that are often taken through drill holes in the bone (proximal phalanx) at the base of the affected toe. The reconstructed toe is then usually stabilized in place with a post-op dressing, or a wire passed across the toe. The toe is then immobilized in position until adequate healing of the soft tissues has occurred. This is often a number of weeks. Following this period of immobilization gentle range of motion exercises are performed combined with a protective shoe. Over time and with a gradual progression in activity patients can usually return to more normal function. However, it can be many months until a full recovery is achieved.
September 30th, 2024