
Calf Muscle Tear
(Gastrocnemius Tear)
Edited by Hossein Pakzad, MD
Summary
Watch Video: Calf Muscle Tears
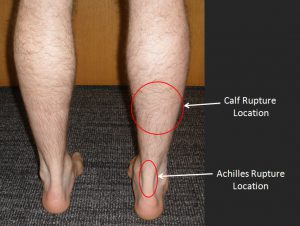
Calf (Gastrocnemius) muscle tears commonly occur in middle-aged recreational athletes while performing actions that require forceful contraction of the calf muscle (ex: basketball, hill running, tennis, etc.). Calf muscle tears have similar symptoms and occur by a similar mechanism to Achilles tendon ruptures. The difference is the location of the injury. Achilles tendon ruptures involve the actual Achilles tendon with pain located just above the back of the heel. Calf muscle tears occur higher up where the muscle belly attaches to the fascia (musculotendinous junction). Figure 1 shows the typical location of each injury. Because of the similarities between the injuries, an Achilles tendon rupture must be ruled out in the diagnosis. Treatment of calf muscle tears is non-surgical. In most instances, initial treatment includes activity modification (limiting muscle-loading activities), wearing a boot (Cam Walker), and using crutches. As the muscle tear heals, physical therapy exercises are utilized to regain full range of motion and muscular strength. Significant improvement can be expected within the first two weeks, but full recovery can take up to 6-8 weeks. It may take many more months to regain muscle mass in the calf that had been atrophied (weakened) due to lack of use.
Figure 1: Typical Location of Calf Tear vs Achilles Tendon rupture
Printable Handout
Clinical Presentation of Calf Muscle Tears
Calf (Gastrocnemius) muscle tears can occur in sports related activities. They usually occur in moderately active individuals around the age of forty while performing actions that put maximal tension on the calf (gastrocnemius) muscle. This injury may be more common in individual who have less consistency in physical activity which can lead to loss of strength and flexibility in the muscles, tendons and ligaments thereby increasing the chance of injury. However, even professional athletes can sustain a calf muscle tear.
The mechanism of injury is very similar to that of an Achilles tendon rupture, which must be ruled out in the diagnosis. Calf tears often occur while performing actions that require forceful shortening (contraction) or sudden lengthening of the calf muscle (ex: basketball, hill running, tennis, “missing a step”, etc.). If we consider classic Achilles tendon rupture the lower end of Achilles tendon injury, the typical Gastrocnemius tear or calf muscle tear happens to the other or higher end of Achilles tendon. The typical location of this injury is where the muscle belly attaches to the fascia (musculotendinous junctions) of the Achilles tendon. This is about 1/3 high in the calf. These tears most commonly involve the inside portion (medial head) of the gastrocnemius muscle as this region is under the greatest amount of tension. Patients with calf muscle tears usually describe a sudden, sharp pain on the inside aspect of the calf. Immediately after suffering a calf tear, patients will walk with a painful limp. Bruising and swelling in the calf area will often develop over the next 24-36 hours.
Physical Examination related to Calf Muscle Tears
Clinical examination of a calf muscle tear will find acute tenderness upon palpation to the entire inside aspect of the calf muscle (medial gastrocnemius muscle). Typically there is bruising associated with this pain and normally the maximum tenderness or location of tear is higher than the bruised area. Depending on the degree of bruising and swelling, a palpable defect in the muscle may be evident.
Stretching of the ankle in an upward direction (dorsiflexion) will produce moderate to severe pain (due to stretching of the torn muscle fibers). Similar pain will be noted with downward ankle motion (ankle plantar flexion), due to the contraction of the torn muscle fibers. These torn calf muscle fibers will produce pain if the patient attempts to perform a calf raise or walk on tiptoes. During the initial phase of the injury, patients will walk with a limp.
As a calf muscle tear can mimic an Achilles tendon rupture, a careful physical exam is essential to differentiate between these two injuries. Achilles tendon rupture occurs below the typical location of a calf muscle tear (Figure 1) and is associated with a palpable defect in the actual Achilles tendon.
Imaging Studies
Plain x-rays may be necessary if your physician wishes to assess the underlying bone. If there is a question as to whether the Achilles tendon is involved, an MRI may be indicated. An MRI is able to accurately assess the soft tissue and differentiate between an injury to the Achilles tendon and the calf muscle tear.
Treatment of Calf Muscle Tears
Treatment of calf muscle tears is usually non-surgical, and dependent upon the individual’s symptoms. In most instances, initial treatment includes activity modification (limiting muscle-loading activities), wearing a boot (Cam Walker), and using crutches. As the muscle tear heals, physical therapy exercises are utilized to regain full range of motion and muscular strength. Significant improvement can be expected within the first two weeks, but full recovery can take up to 6-8 weeks. It may take many more months to regain muscle strength in the calf. Occasionally, excessive scarring will form in the location of the tear. This can cause chronic pain in the area, or render it more likely for future tearing as the fibrotic scar tissue absorbs forces differently than regular healthy muscle tissue.
Initial (Acute Phase) Treatment
Immediately after the injury (first 24-72 hours) treatment should include:
- Relative rest. Limit the use of the injured calf, by limiting standing and walking and possibly using crutches if needed.
- Ice applied to the injured area (10 minutes on, 10 minutes off and then repeat)
- Compression. Light compression with a wrap may be helpful
- Elevation. Elevate the leg at, or slightly above, the level of the heart. For example, by lying on a bed with the foot propped up by a couple pillows.
- Gentle foot and ankle range of motion (ROM) exercises can be carried out as long as the motion is relatively pain-free
- Immobilize the ankle in a neutral position. Studies have shown an increased rate of healing with the ankle braced in a neutral position (ex. foot at a right angle to the lower leg). Your physician may recommend placing your leg in a splint (soft cast) or boot to achieve this position. A splint or boot also serves to protect the injury. In some cases a half inch heel lift to relax the tension behind the calf is appealing to some patients.
Recovery Phase
Once pain free, the patient should progress from gentle plantar flexion (downward motion) exercises against resistance (use of resistance bands), to gradual introduction of stationary cycling, leg presses, and heel raises. Massage techniques can help to decrease swelling and prevent formation of scar tissue.
Maintenance Phase
Once pain-free strength and flexibility have returned, sport-specific activities can be introduced. The long-term goal of rehabilitation is to overcome the increased risk for re-injury by minimizing scar tissue formation and maximizing muscle strength and function. Calf strengthening and calf stretching should continue for several months.
Printable Handout
Edited October 15, 2018
(Previously edited by Paul Juliano, MD and Matthew Buchanan, MD)
mf/ 7.24.18
