
Master Knot of Henry Tenosynovitis
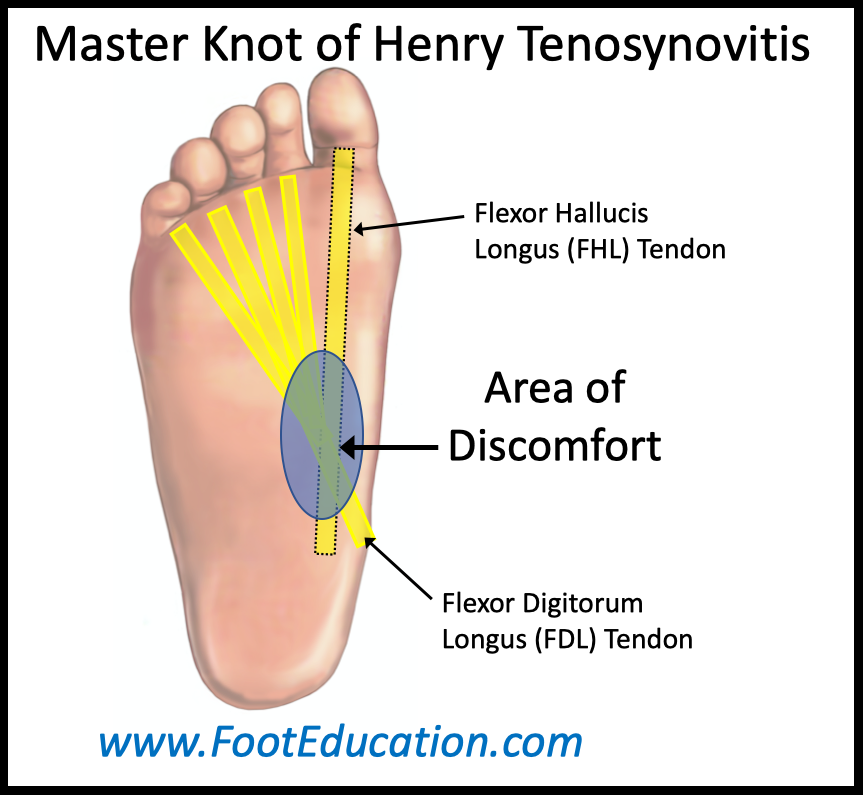
Tenosynovitis of the master knot of Henry causes chronic localized discomfort in the sole of the foot. The master knot of Henry is the area in the sole of the foot (Figure 1) where the tendon that flexes the smaller lesser toes (flexor digitorum longus) crosses over the tendon that flexes the big toe (flexor hallucis longus). Normally these two tendons slide smoothly past each other. However, if irritation or scarring of the two tendons occurs in this area, a localized painful tenosynovitis may occur. This condition can develop gradually without any obvious precipitating event. However, local trauma to the foot often serves to incite this condition.
Physical Exam Findings
Patients with pain originating from a tenosynovitis of the master knot of Henry will have localized discomfort in the sole of their foot where these two tendons cross (Figure 1). Pressing in this area will often re-create the discomfort. Extending the great toe or lesser toes so that the tendons are stretched may also aggravate symptoms.
Imaging of Tenosynovitis of the Master Knot of Henry
Plain weight-bearing x-rays of the foot will usually be normal. Although, they may be helpful to ensure there are no bony or soft tissue prominences that would irritate the tendons as they pass by.
An MRI or ultrasound will allow a closer review of the soft tissues. They may identify thickening of the tendons, swelling of the tendon sheath, and/or fluid around the tendons where they cross. In some instances, there can be some attritional (partial) tearing of one or both of the tendons.
Treatment of Tenosynovitis of the Master Knot of Henry
Initial treatment of tenosynovitis of the master knot of Henry includes stopping any aggravating activities and using comfort shoes with a soft orthotic insert. This is designed to minimize further irritation to the area.
Physical therapy and a home exercise program can be very helpful to mobilize the tendons; break up any associated scar tissue; and decrease the associated inflammation. A therapy program over 4-8 weeks that also includes exercises that patients do daily at home often leads to a notable improvement or a resolution of symptoms.
In patients with recalcitrant symptoms, a local injection of corticosteroids or PRP maybe tried to settle the inflammation in this area.
Surgery is rarely indicated for symptomatic tenosynovitis of the master knot of Henry unless there is a physical impingement of bone or soft tissue that is directly irritating the tendons. In general, it is best to try and avoid placing an incision on the sole of the foot as scarring in plantar area may create debilitating persistent symptoms.
August 28th, 2024