
Low-Lying Peroneus Brevis Muscle Belly and Peroneus Quartus Muscle as a Source of Lateral Ankle Pain
A low-lying peroneus brevis muscle belly or a peroneus quartus muscle are both potential sources of chronic pain in the back outside part of the ankle (posterolateral ankle). The peroneus brevis muscle belly normally ends about 2 cm before the tip of the fibula, which is the prominent bone on the outside of the ankle. However, it has been reported that in up to 53% of patients this muscle belly extends to, or past, the tip of the fibula (Figure 1). This figure increases to up to 87% of patients with peroneal pathology, such as peroneal tendonitis.
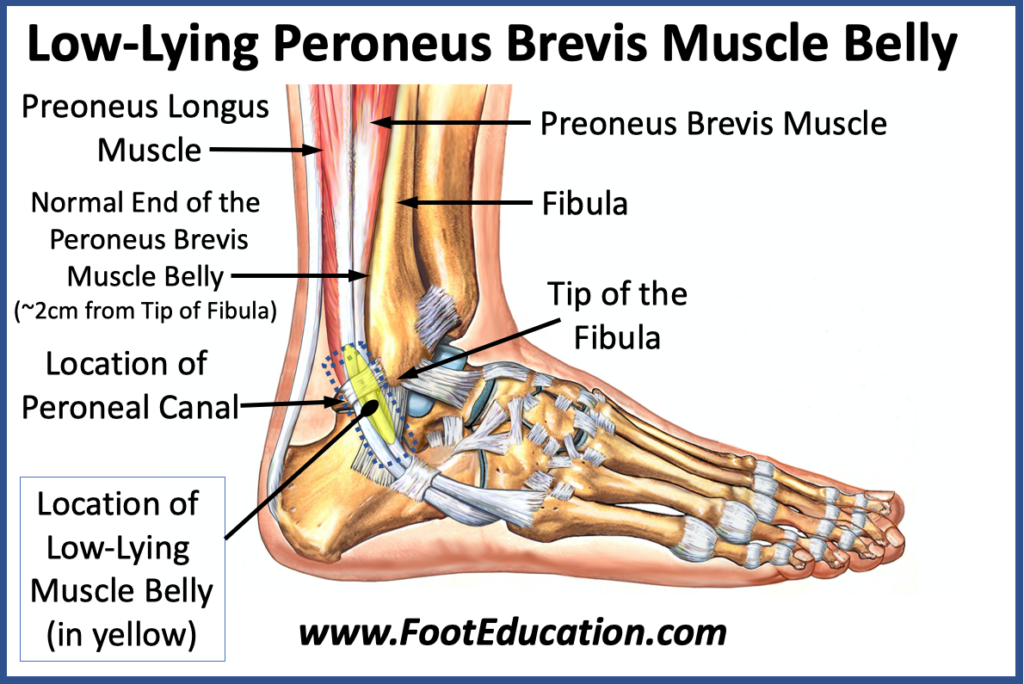
The peroneus quartus is a small extra muscle that is present in the outside back part of the ankle in about 6% of people. It can create problems similar to a low-lying peroneus brevis muscle belly in that it also takes up space within the peroneal canal. The peroneal canal is the small space immediately behind the bone on the outside of the ankle, that the two peroneal tendons run through. The peroneus quartus originates from the peroneus brevis muscle belly, but it is considered a separate muscle because it has its own distinct tendon that attaches to the outside of the heel bone.
Symptoms Associated with a Low-Lying Peroneus Brevis Muscle Belly
Affected patients will often report pain in the outside back part of the ankle. This localized discomfort is often aggravated by activities such as walking or running. A low-lying peroneus brevis muscle can cause discomfort in younger patients, or potentially contribute to the development of peroneal tendonitis in patients as they get older.
Theories on How a Low-Lying Peroneus Brevis Muscle Belly Creates Pain
Symptoms of pain and discomfort are believed to arise from crowding of the peroneal canal. The extra muscle bulk either from a low-lying peroneus brevis muscle or the presence of a peroneus quartus muscle is believed to create pain from increased pressure on the muscle tissue. The crowding of structures within the canal may also lead to peroneal tendonitis and longitudinal tearing of the peroneal tendons over time. There are also some reports of the increased crowding in this space predisposing to chronic peroneal tendon subluxation.
Imaging Studies
Plain x-rays of the foot and ankle do not normally identify any obvious pathology.
An MRI can usually identify evidence of a muscle belly that extends more distally than normal. However, it cannot identify dynamic subluxation of peroneal tendons.
An ultrasound can usually identify a low-lying peroneus brevis muscle or a peroneus quartus muscle. It may also be able to more clearly delineate the effects, such as internal subluxation of the tendons, that the extra muscle bulk has on the surrounding tendons of the peroneus longus and peroneus brevis.
Treatment
Conservative treatment can be quite helpful for patients with relatively mild symptoms related to a low-lying peroneus brevis muscle belly. Physical therapy to mobilize the soft tissue in this area and improve balance around the ankle can be helpful. Some patient may also benefit from the use of an ankle brace or ankle taping. Activity modification and occasional use of anti-inflammatory medications can also be helpful.
Surgical Treatment of a Low-Lying Peroneus Brevis Muscle Belly
For patients with more persistent symptoms or severe symptoms. Surgery may be necessary. Surgery typically involves exposing the tendons and the low-lying muscle belly within the peroneal canal. This is done by making an incision on the back outside part of the ankle. The extra muscle belly is resected to free up more space within the peroneal canal. The surgeon, then ensures that all of the tendons are running freely and that all bleeding has been stopped. The wound is then closed. Once adequate wound healing has occurred the patient can start a physical therapy program. Patients often do quite well after undergoing this procedure, although recovery can be prolonged.
The usual surgical risks are of concern including:
- Surgical Infection
- Wound healing issues
- Persistent discomfort
- Sural neuritis: This is of particular concern with this surgery as the sural nerve is quite close by and needs to be protected throughout the operation.
February 1st, 2024