

Lateral Column Lengthening
Edited by Kalpesh Shah FRCS
Indications
A lateral column lengthening procedure is indicated for patients with acquired adult flatfoot deformity, where the front part of the foot is splayed out to the side. This procedure is often combined with a medializing calcaneal osteotomy, (often referred to as the “All American procedure”), as a technique for adjusting acquired adult flatfoot deformity. The lateral column lengthening procedure provides a powerful correction in patients with flatfoot foot deformities, however, though it is a procedure with clear advantages, there are also potential disadvantages.
Procedure
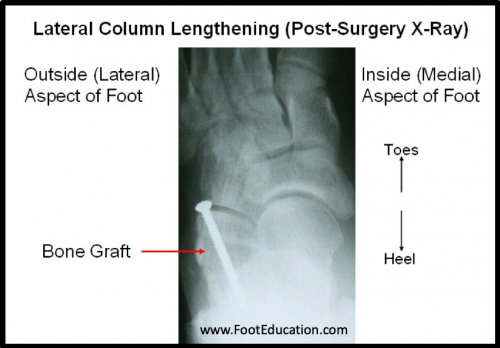
The lateral column is made up of the calcaneus, the cuboid, and the fourth and fifth metatarsals (Figure 1). Therefore, the lateral column lengthening procedure involves lengthening this region. There are two general ways of doing a lateral column lengthening, both of which involve taking a bone graft and inserting it into the lateral column. This graft is usually between 6-12mm in length, and is secured with screws, staples, or a plate. The bone graft is a trapezoidal bone piece and can be either taken from the top aspect of the pelvis (iliac crest) or, in some instances, from a cadaver.
Figure 1:


One way of performing this procedure is by cutting the bone (osteotomy) through the front part of the calcaneus. An osteotomy (bone cut) of the calcaneus is performed right before the calcaneal-cuboid joint, which is then spread about 7-10 mm so that the bone graft can be inserted, in order to lengthen the column (Figure 2).
Figure 2: Lateral column lengthening through the calcaneus

Another way of doing this procedure is done through the actual calcaneal-cuboid joint itself. The bone graft is inserted in the joint, which serves as a joint fusion while also lengthening the lateral column.
A lateral column lengthening procedure is a very powerful procedure, since it can dramatically change the shape of the foot. The advantages of this procedure include the ability to take a pronounced flatfoot deformity and turn it into a near normal looking foot. However, the disadvantages include the potential of creating a stiffer foot; possibly overcorrecting the foot (which may lead to more symptoms); and a higher rate of specific complications, such as painful hardware, sural nerve irritation, and nonunion.
Recovery
0 to 6-10 weeks
For the first 6-10 weeks, the patient is either non-weight bearing or limited weight bearing through the heel, until the bone graft has healed.
6-10 weeks to 12-16 weeks
For the next 4-6 weeks (assuming the bone graft has healed), the patient can weight bear as tolerated in a cast boot. At the 10-16 week mark, the patient can then transition into a shoe.
About 75% of the recovery occurs within the first 5-6 months. However, full recovery can take up to 18 months.
Potential General Complications
Potential Specific Complications
- Sural Nerve Injury: Since the sural nerve is located around the region where the surgery is performed, it may get injured, which may cause numbness, irritation, and/or pain.
- Nonunion: The bone graft placed to expand the lateral column may not heal. This could necessitate further surgery. It seems that the rate of non-union may be higher when the bone graft is placed in the calcaneal-cuboid joint, compared to through the calcaneus itself.
- Painful Hardware: The screws used to secure the bone graft may become painful, requiring removal. This occurs in about 15-20% of patients.
- Over Correction/Under Correction: Determining the extent of correction required can be challenging for the surgeon. If the foot ends up in less than an ideal position, the patient may end up with more symptoms.
Previously edited by Sam Dellenbaugh, MD
Edited February 11, 2020
mf/4.23.18